Introduction: Why Trying to Be Healthier Can Make You Feel Worse

Sleep score, step count, heart rate, caloric intake, macronutrient ratios. Every biological data point tracked, every superfood and detox and biohacking protocol attempted. And yet — a small deviation in the numbers produces something disproportionate: distress, self-reproach, a meal that can’t be enjoyed, rest that arrives wrapped in guilt. The voice saying more correctly, more efficiently doesn’t stop.
This is not health consciousness. It is a state in which the pursuit of health has begun generating its own kind of damage. And the structure driving it did not originate with you.
Session 1: When “Eating Right” Becomes Compulsion

The transformation of health behavior into compulsion tends to happen without announcement. It begins as reasonable choices — reducing processed food, building an exercise habit, improving sleep. The problem emerges when those behaviors detach from their original purpose and begin functioning as proof of something: not care for the body, but evidence of a correctly managed self.
The self-disgust after eating something deemed impure. The disproportionate guilt following a deviation from the plan. The gradual migration of food choices into the territory of self-evaluation. These are not phenomena exclusive to clinical eating disorders — they are the edge of a pattern that contemporary wellness culture produces broadly. Physician Steven Bratman, who coined the term orthorexia nervosa in 1997, was describing a pathological fixation on eating correctly: centered not on caloric restriction or body weight but on the purity and moral rightness of food. What he named at the clinical extreme has a much wider distribution.
When health behavior becomes compulsion, the body is no longer the point. The body has become an apparatus for demonstrating correctness — and the pursuit of health has quietly become a different project entirely.
Session 2: Practice — From Monitoring to Dialogue
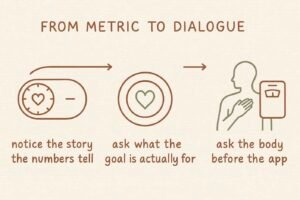
This practice is not about abandoning health goals. It is about changing the quality of the relationship with the body — moving from external surveillance toward something more reciprocal.
STEP 1: Notice the Story the Numbers Are Telling About You
When the thought arrives — I didn’t hit my target, I went over my limit — and the self-criticism that follows — I have no discipline, I failed again — pause before receiving it as fact.
My mind is running the story that connects a health metric to my worth as a person.
Hear it as a commercial voiceover passing through — present, audible, not necessarily true. Recognizing it as a story rather than a verdict doesn’t eliminate the discomfort. It creates a gap between the number and the judgment. That gap is where a different response becomes possible.
STEP 2: Ask What the Goal Is Actually For
When the pull toward a specific target intensifies — body fat percentage, daily step count, sleep score — pause to locate what the target is actually serving.
Why am I pursuing this? What is on the other side of it?
The desire to have energy for the people and activities that matter, to remain mobile and capable as the years pass, to treat the body with care rather than suspicion — these values exist independently of any metric. They can be acted on today, regardless of what the numbers say. A goal can be failed. A value cannot. Even after a day when nothing went according to plan, the next choice can still move in the direction of something genuinely cared about.
STEP 3: Ask the Body Before Asking the App
Before checking any monitoring device, build the habit of directing a question inward first. Before eating: what is the body actually asking for right now? Before exercise: is today asking for intensity, or for something quieter? Before sleep: is the body signaling that it needs rest, independent of what the sleep tracker will say?
This is not a rejection of measurement. It is a change in sequence — one question to the body before one glance at the screen. That small reordering gradually shifts the balance between external metric and internal signal, restoring some weight to the information the body has been generating all along.
Session 3: When Did Health Become a Moral Category?
The Social Manufacture of Health Obsession
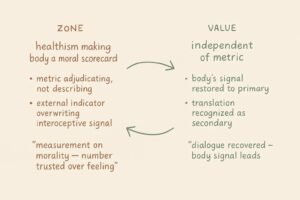
When Steven Bratman named orthorexia in the late 1990s, he was describing a clinical edge case. What he was also observing, without necessarily naming it as such, was the individual-level expression of a structure sociologist Robert Crawford had identified nearly two decades earlier. Crawford’s concept of healthism — introduced in 1980 — describes the ideological positioning of health as a personal moral responsibility. Within this framework, being healthy becomes evidence of self-discipline and virtue; being unhealthy becomes evidence of insufficient will or effort. Health disparities that are structurally produced disappear from view, reframed as the cumulative result of individual choices. In a healthist framework, the body is a project, and its condition is a verdict on the person managing it. The disproportionate distress produced by a deviation in health metrics is not a quirk of individual temperament. It is the predictable internal experience of living inside an ideology that has made health into a moral scorecard.
The Metrics Made the Morality Visible
Sociologist Deborah Lupton’s analysis of Quantified Self culture documents what happens when healthism meets measurement technology. Wearable devices and health applications render the body’s state as continuous real-time data. This appears, on the surface, to be neutral information. But data always comes with reference ranges, and reference ranges always come with the implicit categories of achievement and failure. When the moral framework of healthism is already in place, the step count that falls short becomes evidence of laziness, the sleep score that declines becomes a record of self-management failure. The metric is no longer describing the body. It is adjudicating it. The paradox in which more monitoring produces more anxiety rather than more reassurance is not a design flaw. It is the structural consequence of placing a measurement system on top of a moral one.
When the Data Became the Body
Neuroscientist Sarah Garfinkel’s research on interoception — the brain’s processing of signals from inside the body, including organ state, muscle tension, and breath — established that this internal signal system underlies emotional recognition, decision-making, and the basic sense of physical wellbeing. What chronic health monitoring produces is something distinct from the gradual narrowing produced by sedentary culture. It is active overwriting. When the step counter says you need more and the body says you’re tired, the counter tends to win. When the sleep application reports insufficient deep sleep and the body reports feeling rested, the report tends to override the sensation. Chronic dependence on external indicators trains the brain to treat internal signals as secondary — less reliable, in need of correction by the data. When the number is trusted more than the feeling, the conversation with the body has effectively ended. The number was always a translation of the body, not the body itself. And in every translation, something is lost.
Conclusion: The Number Was Never the Body

The wellness industry will generate new metrics tomorrow. The moral logic of healthism will keep processing deviations as failures. The internal signal will keep losing ground to the external indicator. The structure does not change.
But the question what is my body actually telling me right now cannot be answered by any application. Asking it once — before reaching for the device — is a small reordering of trust. Over time, that sequence restores some of what the monitoring displaced.
The number was never the body. It was a translation — and something was always lost.
KEY TERMS
Orthorexia Nervosa
Physician Steven Bratman’s 1997 term for a pathological fixation on eating correctly — centered not on caloric restriction or body weight but on the purity and moral rightness of food. Deviation from the self-defined correct diet produces disproportionate guilt and self-reproach. Not an isolated clinical condition but the visible edge of a pattern that contemporary wellness culture generates more broadly: the migration of health behavior from bodily care into moral self-proof.
Healthism
Sociologist Robert Crawford’s 1980 concept describing the ideological positioning of health as a personal moral responsibility. Being healthy signals virtue and self-discipline; being unhealthy signals insufficient effort or will. Structural contributors to health disparities become invisible, reframed as the result of individual choices. The framework within which health metrics function as moral verdicts rather than descriptive data — and within which deviations produce distress disproportionate to their actual physical significance.
Quantified Self
Sociologist Deborah Lupton’s analysis of the culture produced by wearable devices and health applications that render the body’s state as continuous real-time data. When placed on top of the moral framework of healthism, neutral measurement becomes moral adjudication: the shortfall is laziness, the decline is failure. The structural explanation for why increased monitoring tends to produce increased anxiety rather than reassurance — the paradox is not a design flaw but a predictable consequence of combining a measurement system with a moral one.
Interoceptive Override
The process, grounded in neuroscientist Sarah Garfinkel’s interoception research, by which chronic dependence on external health indicators trains the brain to treat internal bodily signals as secondary and less reliable. Distinct from the gradual narrowing produced by sedentary culture: this is active displacement. When the external metric consistently overrides the internal sensation, the brain gradually reweights its trust toward the data and away from the feeling. The conversation with the body ends not with a decision but with accumulated habit.
Defusion
The capacity to notice that the story connecting a health metric to personal worth has fused with one’s experience, and to receive it as a story rather than a verdict. Hearing the self-critical thought as a commercial voiceover passing through — present but not authoritative — creates the gap between number and judgment in which a different response becomes available.