Introduction: The Exhaustion Isn’t From Feeling Too Much

After listening to someone’s pain, you’re drained. After a difficult conversation, their anxiety is still with you hours later. Every time you hold space for someone in pain, something in you diminishes — quietly, without a clear cause.
The instinct is to explain this as being too sensitive — and to conclude that the solution is to feel less. Both the diagnosis and the prescription are wrong.
Most empathy fatigue comes not from the quantity of feeling but from the dissolution of the role boundary — the point at which the other person’s experience stops being something you’re present with and becomes something you’re carrying. That shift is where the drain originates.
Session 1: What a Role Boundary Actually Is

Doctor, counselor, teacher, parent, friend — these are all roles. A role is a structure that makes a particular kind of engagement possible. The role is what allows you to move toward another person’s suffering without being destroyed by the encounter.
But roles have two layers. Occupying a role and being completely absorbed by it are different things. A surgeon who fully merges with a patient’s pain cannot operate. A counselor who absorbs a client’s anxiety as their own loses the capacity for judgment. The role itself requires a degree of separation between the person performing it and the experience being witnessed.
Sociologist Erving Goffman called the space between these two layers role distance — the capacity to fully inhabit a role while retaining the awareness that you are not identical to it. This is not detachment. It is the structural condition that makes the role sustainable over time.
Empathy fatigue is what happens when role distance collapses.
Session 2: Three Steps for Recovering Role Distance
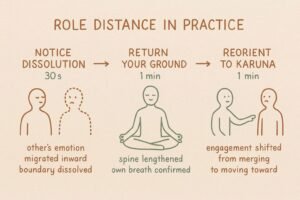
Use this practice when the signs of empathy fatigue are already present — feeling drained after a conversation, carrying the other person’s emotional state, wanting to escape the interaction.
STEP 1: Notice the boundary dissolution (30 seconds)
Register what is actually happening internally.
Their anxiety has become my anxiety.
I feel responsible for resolving their situation.
Their pain is producing pain in me.
Without judgment. Simply confirm that the role boundary has dissolved — that the other person’s experience has migrated inward and is being processed as your own.
STEP 2: Return to your own ground (1 minute)
Use physical sensation to re-establish the boundary.
Lengthen the spine, feel the contact with the chair or floor.
Return attention to your own breath — yours, not theirs.
Confirm internally: I am present with this person’s suffering. It is not mine to carry.
This is not distance from the person. It is a return to your own standing position — from which genuine presence becomes possible again.
engagement (1 minute)
From the recovered position, shift the direction of engagement.
From feeling what they feel toward what can I offer from where I am.
From suffering alongside toward moving toward their suffering with warmth.
This is the practical structure of Karuṇā — moving toward suffering without merging with it.
Session 3: Role Distance, the Cost of Emotional Labor, and Why Burnout Is a Structural Problem
The understanding that empathy fatigue is a boundary problem rather than a sensitivity problem is supported from both sociology and clinical psychology.
Erving Goffman’s concept of role distance, developed in Encounters (1961), arose from observations of surgeons. Goffman noticed that surgeons in the operating room would joke, make casual remarks, maintain an atmosphere of lightness during serious procedures. The conventional interpretation was unprofessionalism. Goffman’s analysis was the opposite: the levity was a form of role distance — a mechanism by which the surgeon demonstrated, to themselves and the team, that they were more than the role in which they were momentarily submerged. Role distance is not indifference to what the role requires. It is the maintenance of a self that exceeds the role, which is what prevents the role from consuming the person performing it. In care contexts, the implication is specific: full merger with the suffering being witnessed does not deepen the care. It erodes the capacity to continue providing it.
Arlie Hochschild’s concept of emotional labor, developed in The Managed Heart (1983), describes the work of managing emotional states as part of occupational performance. Hochschild distinguished between surface acting — managing the external expression of emotion while internal experience differs — and deep acting — attempting to actually produce the required internal emotional state. Deep acting is significantly more costly. The empathic response that produces fatigue tends to involve a form of deep acting: not only appearing to feel what the other person feels, but attempting to actually reproduce their emotional state internally. This is the most resource-intensive form of emotional engagement — and it is often exactly what people mean when they say they want to really be there for someone.
Charles Figley’s clinical work on secondary traumatic stress — the emergence of trauma-like symptoms through repeated exposure to others’ traumatic material — identified that risk does not correlate primarily with the sensitivity of the individual practitioner. It correlates with structural conditions: insufficient supervision, no mechanism for role transition, absence of self-care structure, and — most relevantly here — the absence of role distance. People who develop secondary traumatic stress are not those who feel too much. They are those placed in conditions where the boundary between their own experience and the experience they are witnessing is systematically eroded. The implication shifts the problem from a personal failing to a structural one — which is where the intervention belongs.
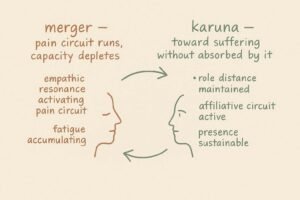
Richard Davidson’s research showed that empathic resonance and compassionate engagement activate different neural circuits: the former recruits pain-processing regions and produces fatigue; the latter recruits the affiliative and reward systems and maintains engagement capacity. Goffman’s sociological role distance and the neural structure of Karuṇā are describing the same functional requirement from different angles — the capacity to be fully present with suffering without being absorbed by it.
Conclusion: The Distance Is What Makes the Care Possible
Next time role distance collapses — notice it.
Return to your own ground. Return to your own breath. From that position, move toward the other person’s difficulty.
Toward, not into.
Compassion moves toward the suffering. Empathy merges with it. The difference is what keeps you standing.
KEY TERMS
Role Distance
Erving Goffman’s concept from Encounters (1961): the capacity to fully inhabit a role while retaining the awareness that one is not identical to it. Observed in surgeons who maintained levity during operations — not as unprofessionalism, but as a mechanism for preserving a self that exceeds the role. In care contexts: full merger with the suffering being witnessed erodes rather than deepens the capacity for care. Role distance is the structural condition that makes sustained engagement possible.
Emotional Labor
Arlie Hochschild’s concept from The Managed Heart (1983): the work of managing emotional states as part of occupational performance. The distinction between surface acting (managing emotional expression) and deep acting (attempting to produce the required internal state) is critical — deep acting is significantly more resource-intensive. Empathic responses that reproduce the other person’s emotional state internally are a form of deep acting, and represent the most costly available form of emotional engagement.
Secondary Traumatic Stress
Charles Figley’s clinical description of trauma-like symptoms arising from repeated exposure to others’ traumatic material. Risk correlates not with individual sensitivity but with structural conditions — absence of supervision, role transition, and role distance. Reframes empathy fatigue as a structural problem rather than a personal failing, which is where the relevant intervention belongs.
Karuṇā and Role Distance
The structure of compassionate engagement — moving toward suffering without merging with it — maps onto Goffman’s role distance from a different direction. Both describe the same functional requirement: full presence with suffering that does not dissolve the boundary between witness and experience. Richard Davidson’s neuroscience research confirms that this distinction has a measurable neural basis — empathic resonance and compassionate engagement recruit different circuits with different sustainability profiles.
Defusion
See Guide 5. Role distance sometimes triggers a conviction: I don’t really care, or real presence means feeling everything they feel. Recognizing that conviction as a thought — not an accurate description of care — and returning to the physical recovery in STEP 2 is defusion applied to the belief system that makes role distance feel like betrayal.