Introduction: Caring Continuously and Losing Yourself Are Not the Same Thing

Keeping going for someone who matters. Still moving even when exhausted, because right now they come first.
That dedication is real. But care coming from a depleted source gradually becomes something else — irritation, obligation, hollow motion.
The care that comes from a depleted source eventually stops resembling care at all.
Caring for yourself is not selfishness. It is the condition that makes sustained care possible.
Session 1: The Structure of Depletion and the Dissolving of Boundaries

Caregivers deplete not because their love is insufficient but because caregiving places simultaneous load across multiple layers — physical, psychological, social, economic — continuously and at once.
At the center of that depletion is the dissolution of boundaries through empathy. When another person’s suffering is felt as one’s own, continuously, the distinction between self and other begins to thin. The caregiving role gradually occupies the whole of the self-concept, and the self outside of the role becomes harder to locate. This is what accelerates the depletion.
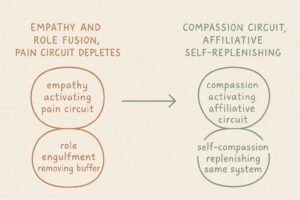
Empathy — emotional merging with another’s experience — and compassion — the intentional movement toward another’s suffering while remaining present as oneself — use different neural circuits. Empathy crosses the boundary and merges; it depletes. Compassion maintains the boundary and moves toward; it can be sustained. What caregivers need is not deeper empathy but the shift to a compassion-based circuit.
Session 2: Practicing Care Toward Yourself
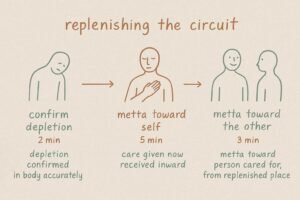
STEP 1: Confirm the current state of depletion (2 minutes)
Is there fatigue somewhere in the body right now? Behind the eyes, in the shoulders, around the chest.
Rather than evaluating it as I’m tired, confirm it as this is present in the body right now. Knowing the state of depletion accurately is where care begins.
STEP 2: Direct Mettā toward yourself (5 minutes)
Toward the self that has been doing the caring, direct quiet intention.
May I receive some of the care I have been giving.
May I be as gentle with myself as I try to be with others.
This is the same quality of intention directed toward others, now turned inward. Not a self-centered act — a replenishment of the circuit that makes care possible.
STEP 3: Direct Mettā toward the person you are caring for (3 minutes)
From a slightly replenished place, direct intention toward the person being cared for.
May you be held by more than my effort alone.
May we both find what sustains us.
From a slightly replenished place, notice whether the direction of the intention feels different from when care comes from obligation.
Session 3: Caregiver Burden, Role Engulfment, the Neural Difference Between Empathy and Compassion, and the Conditions for Sustainable Care
Caregiver depletion is not a single phenomenon. It accumulates at different levels simultaneously — and so does the case for compassion as its intervention.
Steven Zarit’s development of the Zarit Burden Interview in the 1980s established the research foundation for understanding caregiver depletion as a multidimensional structure. Zarit and colleagues showed that caregiver burden is not a single form of fatigue but a structure in which physical, psychological, social, and economic costs accumulate simultaneously and reinforce each other. This multidimensionality is what makes caregiver depletion resistant to willpower-based solutions: addressing one layer leaves the others intact and continuing to compound.
The dissolution of self that caregivers frequently describe — the sense of no longer knowing who they are outside the caregiving role — is described by Peggy Thoits’s role identity research. Thoits, whose work on role identity and psychological wellbeing has been published across several decades in Journal of Health and Social Behavior and related outlets, showed that psychological wellbeing is supported by the diversity of role identities a person holds: multiple sources of self-definition provide a buffer when any single role is threatened or fails. Role engulfment — the process by which a single role occupies the entire self-concept — removes that buffer. When caregiving becomes the whole of a person’s identity, the success or failure of the caregiving becomes the measure of self-worth as a whole. Thoits’s research has informed caregiver support practice by identifying the maintenance of non-caregiving identities as a concrete protective factor.
The neural difference between what depletes caregivers and what sustains them is described by Olga Klimecki’s compassion training research. Klimecki and colleagues, in Cerebral Cortex (2013), showed that empathy — processing another person’s suffering as one’s own — activates pain-processing circuitry, and that sustained activation of this circuitry is associated with negative affect and depletion. Compassion training, by contrast, produced activation of affiliative system circuitry — the medial prefrontal cortex and ventral striatum — and was associated with maintained positive affect even in the presence of others’ suffering. The caregiving circuit that depletes is the empathy circuit. The circuit that can be sustained is the compassion circuit.
How self-compassion functions as the mechanism for replenishing that circuit is where Kristin Neff’s research on self-compassion and burnout provides the endpoint. Research on self-compassion across caregiving and helping professions has shown that self-compassion is negatively correlated with burnout. The mechanism connects directly to Klimecki’s circuit findings: directing warmth toward oneself activates the same affiliative system circuitry that compassion toward others activates — it replenishes rather than depletes the care capacity.
Conclusion: The Presence Was the Care

The carer being present, as themselves, is the condition of the care.
Losing yourself in the caring was never what the person needed from you. Your presence was.
KEY TERMS
Caregiver Burden
Steven Zarit’s multidimensional framework, operationalized in the Zarit Burden Interview (developed in the 1980s), describing caregiving load as a simultaneous accumulation across physical, psychological, social, and economic layers that reinforce each other. The multidimensionality explains why willpower-based approaches are insufficient: addressing one layer leaves the others intact. The framework has shaped the design of caregiver support programs across clinical and community settings internationally.
Role Engulfment
Peggy Thoits’s term for the process by which a single role occupies the entire self-concept, removing the buffer that identity diversity provides. When caregiving becomes the whole of a person’s identity, caregiving outcomes become measures of self-worth as a whole. Thoits’s role identity research identifies the maintenance of non-caregiving identities as a concrete protective factor, informing caregiver support practice in clinical and community intervention contexts.
Empathy-Compassion Circuit Difference
Olga Klimecki and colleagues’ finding, from Cerebral Cortex (2013), that empathy activates pain-processing circuitry and is associated with depletion, while compassion training activates affiliative system circuitry and maintains positive affect. The circuit distinction explains why deeper empathy is not the solution to caregiver depletion — and provides the neural basis for compassion training programs designed for caregivers, healthcare workers, and educators.
Self-Compassion and Sustainable Care
Kristin Neff and colleagues’ research showing that self-compassion is negatively correlated with burnout across caregiving and helping professions. Directing warmth toward oneself activates the same affiliative circuitry that Klimecki identified in compassion toward others — replenishing rather than depleting the care capacity. Self-care reframed as a neural condition rather than a moral choice.