Introduction: The Exhaustion Is Not Evidence of Weakness

Somewhere in the middle of a conversation, the other person’s weight became indistinguishable from one’s own. After listening to a friend, a heaviness lingers that didn’t belong to anyone. Someone else’s difficulty lands and stays. A news story from somewhere far away keeps returning.
Maybe I’m just not strong enough to handle this, the thought arrives. But this exhaustion is not a problem with the depth of feeling. It is what happens when the brain’s empathy circuitry becomes saturated inside a structure that asks for care without acknowledging its limits.
Session 1: What Compassion Fatigue Actually Is
When contact with another person’s emotion produces lasting exhaustion, what is operating is not a failure of emotional resilience. It is a structure.
When another person’s pain is observed, neural circuits that partially overlap with the circuits active during one’s own pain become engaged. This is not a choice or a weakness — it is part of how the social brain is built. In ordinary circumstances this overlap is regulated. Under conditions of repeated emotional demand, the circuitry stays activated, and the processing of other people’s distress as one’s own becomes chronic rather than episodic.
What makes this more difficult is the structure surrounding the care itself. Listening, supporting, staying emotionally present — these are frequently expected as the natural expression of love or friendship or professional commitment, without acknowledgment that they constitute a form of labor with limits. When care is defined as something that flows naturally from good character, feeling its limits reads as a failure of character. The exhaustion arrives, and then the self-criticism for being exhausted arrives alongside it.
The depletion is not the result of caring too intensely. It is the result of care being structurally demanded without limit.
Session 2: Practice — Moving From Affective Empathy Toward Compassion
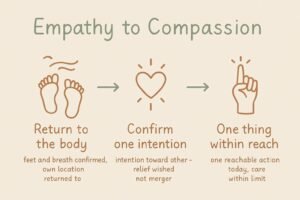
This practice is not about withdrawing care. It is about shifting — gradually, in daily life — from the state of being submerged in another person’s experience to the state of understanding that experience while remaining located in one’s own.
STEP 1: Return to the body
When someone else’s distress produces an emotional response, before anything else, return once to physical sensation.
Are the feet on the floor right now. What is the breath doing. Is there anything in the chest or shoulders.
When being pulled into another person’s emotional state, awareness of one’s own physical experience typically diminishes. Returning to the body is not a withdrawal from the other person. It is the act of confirming where one actually is — which creates the small distance that makes the next step possible.
STEP 2: Confirm one intention toward the other person
After returning to the body, direct one intention toward the person whose distress was encountered.
I would like this person to find some relief from what they are carrying.
This is structurally different from emotional merger. It is not taking on the other person’s pain as one’s own. It is holding attention toward their state — genuinely, with care — while remaining in a separate location. Compassion is not sinking together. It is knowing about the difficulty and reaching toward it from a stable place.
STEP 3: Identify one thing that is within reach today
When the impulse to help arrives, identify one specific thing that can actually be done today.
What is one thing I can offer this person today. Everything else is beyond what today can hold.
The desire to resolve everything comes from care. But the attempt to resolve everything is how the depletion cycle builds. Selecting one reachable action is not the abandonment of care. It is the condition under which care can continue.
Session 3: The Exhaustion Came From Being Asked Without Limit

Care had been made invisible as love
Sociologist Arlie Hochschild’s concept of emotional labor established that the management of feeling — sustaining emotional availability, suppressing one’s own responses, remaining present to others’ distress — functions as a form of labor that is professionally and socially demanded. Philosopher Eva Kittay’s concept of dependency work deepens this framework: human beings universally experience dependency, and the labor of caring for those who are dependent forms the foundation of social life — yet this labor has been systematically rendered invisible by being framed as the natural expression of love rather than as work with recognizable limits and costs. When listening, supporting, and staying emotionally present are defined as what caring people simply do, the experience of those activities’ limits reads not as a reasonable boundary but as a personal failing. Compassion fatigue is not the result of being an unusually sensitive person. It is the predictable result of care being demanded as though it were limitless — and of the person providing it having no socially sanctioned language for the limit.
The nervous system was built to partially merge — and under repeated demand, the boundary became unreliable
Neuroscientist Jean Decety’s research on self-other overlap demonstrated that observing another person in pain activates neural circuits that partially overlap with those engaged during one’s own pain experience. This overlap is not a design flaw or a sign of insufficient emotional regulation. It is a feature of the social nervous system — the mechanism through which other people’s states become legible and motivate prosocial response. Under ordinary conditions, this overlap is modulated: the shared activation occurs, and the distinction between self and other is maintained alongside it. Under conditions of repeated emotional demand — when the circuits are called upon continuously without recovery time — chronic activation sets in. When affective empathy becomes saturated in this way, the cognitive distance required for the shift toward compassion becomes difficult to maintain. The state of sinking together with another person’s distress is not a moral failure. It is what the nervous system does when the self-other boundary has been worn down by use without repair.
A different circuit produced warmth rather than depletion
Neuroscientist Olga Klimecki’s research on compassion training introduced a finding that reframes what is neurologically possible. Affective empathy — processing another’s distress as one’s own — when sustained over time, produces increasing negative affect and is associated with emotional exhaustion. Compassion — holding awareness of another’s suffering alongside the intention that it be relieved — activates a neurologically distinct circuit, one associated with positive affect, warmth, and reward rather than depletion. This shift does not happen automatically. It is produced through practice: repeated activation of the intention toward the other’s relief, in the context of remaining located in one’s own experience. Recognizing the limit of what care can do today is not the end of caring. It is the structural condition under which care remains available.
Conclusion: The Care Can Continue. Recognizing the Limit Is What Makes It Possible

The social structure that demands care as love — without acknowledging it as labor with limits — continues. The neural overlap between self and other that makes another’s pain partially one’s own remains a feature of the nervous system. Affective empathy saturation will keep occurring under conditions of repeated demand.
But the shift from the circuit that depletes toward the one that sustains is available in any encounter where the pull toward merger begins. That shift is not a withdrawal from caring. It is the structure that makes caring last.
The exhaustion was never proof of caring too much. It was proof that the caring had been asked for without limit.
KEY TERMS
Invisibilization of Dependency Work
Eva Kittay’s concept describing how the labor of caring for those who are dependent — universally necessary, socially foundational — has been rendered invisible by being framed as the natural expression of love rather than as work with recognizable limits. Combined with Hochschild’s emotional labor framework, this explains the structure in which care is demanded without limit and the experience of that limit reads as personal failure. The social basis for understanding compassion fatigue as a structural condition rather than an individual weakness.
Self-Other Overlap
Jean Decety’s neuroscientific finding that observing another person in pain activates neural circuits that partially overlap with those engaged during one’s own pain. A feature of the social nervous system, not a failure of regulation. Under ordinary conditions this overlap is modulated. Under repeated emotional demand without recovery, the self-other distinction becomes less reliable — and the shift toward compassion requires more deliberate activation. The neurological basis for understanding why another’s pain becomes one’s own under conditions of sustained care.
Affective Empathy Saturation
The state produced when the neural circuits engaged in processing another’s distress as one’s own are chronically activated without recovery. Results from the combination of the self-other overlap’s structural tendency and the social demand for unlimited care. In saturation, the cognitive distance required for the shift toward compassion becomes difficult to maintain, and the depletion cycle stabilizes. The neurological description of compassion fatigue.
Compassion Training
Olga Klimecki’s finding that compassion — holding awareness of another’s suffering alongside the intention that it be relieved — activates a neurologically distinct circuit from affective empathy, one associated with warmth and positive affect rather than depletion. The shift does not occur automatically; it is produced through deliberate practice. Returning to one’s own body, confirming the intention toward the other’s relief, and identifying one reachable action are the minimum conditions for this circuit to become reliably available.
Sustainable Boundary of Care
The practical principle of identifying what care can actually reach today and distinguishing it from what it cannot. Not the abandonment of care but the structural condition under which care remains available over time. The attempt to resolve everything produces the depletion cycle; the selection of one reachable action closes the loop between genuine concern and sustainable engagement. The individual-level response to the structural invisibilization of dependency work’s limits.