Introduction: The Numbness Is the Signal. The Suffering Comes After.
Partway into a sitting session, the legs go numb — and the first impulse is to move. Most people treat this as an interruption, a sign that the practice has ended.
But what pain neuroscience shows is that the sensation of pain and the suffering of pain are separate processes. The signal arriving from the leg is one thing. Whether that signal becomes suffering depends on what happens to it on the way.
Using leg numbness as an object of observation makes it possible to watch this process directly.
Session 1: Pain Is Built From Two Layers
There is a moment — just before moving — when something can be noticed. The sensation is there. But is it actually unbearable? Or is the reaction to it what has become unbearable?
Nociceptive input — the signals generated by tissue pressure, stretch, and oxygen deprivation in the muscles and nerves — travels through the spinal cord to the brain. But how much pain is experienced is not determined by signal strength alone. Attention, emotional state, expectation, past experience — these intervene in the processing of the signal and alter the intensity of what is felt.
Pain experience has two layers. The first is sensation: the neural signal itself. The second is suffering: the evaluation, resistance, and emotional response that the signal accumulates on its way into conscious experience.
In most cases, what we call pain is these two layers arriving together, indistinguishable. The practice here is to observe them separately.
Session 2: Four Steps

When numbness or pain arrives, receive it as the beginning of a different observation rather than the end of the practice.
STEP 1: Pause before reacting (30 seconds)
The moment pain is noticed, hold the impulse to move — not prohibit it, but hold it for one beat. Confirm internally: *a pain signal is arriving.* The pause is the whole of this step.
STEP 2: Observe the sensation specifically (1–2 minutes)
Rather than registering the sensation as pain, observe its actual characteristics.
Location: where, and over what area?
Quality: numbness, tingling, heaviness, heat — what combination?
Intensity: on a scale of one to ten, right now?
Change: compared to thirty seconds ago, is anything different?
Don’t try to change the sensation. Just describe what is actually there.
STEP 3: Separate the sensation from the response (1–2 minutes)
Distinguish the sensation itself from the reaction to it.
Is the sensation of numbness a different thing from the feeling of not wanting it?
Is the pain signal a different thing from the thought that it won’t stop?
Is the sensation changing? Is the resistance holding it fixed?
If the separation isn’t clear, that’s fine. Moving attention in this direction is the practice.
STEP 4: Choose consciously (30 seconds)
After observing, select the next action deliberately.
If the sensation is within an observable range, continue.
If it is too strong, adjust the posture.
Either choice is a considered decision, not a failure.*
⚠️ Important: Distinguish the type of pain
Numbness and muscular tension in the legs and feet can serve as objects of observation. However, if burning, sharp, or radiating pain arises in the lower back, buttocks, or spine, change position or end the session immediately. This type of pain — involving risk to the intervertebral discs, sciatic nerve, or deep musculature — is not an object of observation. It is the body’s signal to stop.
Session 3: Gate Control Theory, the Two-Layer Processing of Pain, and the Distinction Epictetus Made Two Thousand Years Ago
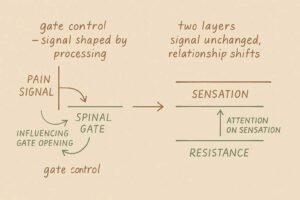
In 1965, Ronald Melzack and Patrick Wall published what became known as gate control theory — a proposal that fundamentally changed how pain was understood. The prevailing model before this was essentially a pipeline: tissue damage generates a signal, the signal travels to the brain, the brain registers pain in proportion to the damage. What Melzack and Wall showed was that the spinal cord contains a gating mechanism — a neural structure in the dorsal horn that regulates how much pain signal passes through to the brain. And critically, this gate is not controlled only by the physical intensity of the signal. Attention, emotional state, expectation, and prior experience all influence it. The soldier who doesn’t notice a wound until the battle is over; the way anxiety amplifies pain and distraction diminishes it — these are the gate mechanism operating. Gate control theory has since been refined and extended, particularly through Melzack’s later development of the neuromatrix model, which emphasizes the brain’s active role in constructing pain experience. The core insight — that pain is not a fixed readout of tissue damage but an experience formed through processing — remains foundational to contemporary pain neuroscience.
The clinical application of this insight is visible in Jon Kabat-Zinn’s early work with chronic pain patients in the MBSR program. The consistent observation was this: separating the sensation of pain from the evaluation of and resistance to that sensation — attending to the former while loosening the grip of the latter — could change the experience of suffering even when the underlying sensation remained unchanged. Reducing pain and changing the relationship to pain are different interventions. The second is what mindfulness practice approaches, and it is consistent with what gate control theory describes: the processing layer, not the signal itself, is where attention can intervene.
From philosophy, Epictetus made a related distinction at the opening of the Enchiridion — written approximately two thousand years before gate control theory. Some things are within our power, he wrote, and some are not. The pain signal arriving from the leg falls in the second category. The evaluation of that signal, and the response to it, fall in the first. What Epictetus described as a philosophical principle — the separation between event and judgment — is the same distinction that gate control theory describes as a neurological fact, and that this practice makes available as direct experience. The leg provides the signal. What the signal becomes is shaped by what the mind does with it.
Conclusion: The Signal Arrives. What Happens Next Is Not Fixed

The legs go numb. There is one beat — before the impulse fires — where something can be seen. Not fixed, not managed. Just seen for what it actually is: a signal, moving through a system that is still deciding what to do with it.
The sensation was always just the signal. The suffering was what happened to it on the way up.
The space between the signal and the response is not empty. It is where the practice lives.
KEY TERMS
Gate Control Theory
Ronald Melzack and Patrick Wall’s 1965 proposal that a gating mechanism in the spinal cord’s dorsal horn regulates how much pain signal reaches the brain — and that this gate is influenced not only by signal intensity but by attention, emotional state, expectation, and prior experience. The foundational insight: pain is not a fixed readout of tissue damage but an experience formed through processing. Melzack later developed this into the neuromatrix model, emphasizing the brain’s active role in constructing pain experience. Gate control theory remains the basis of contemporary pain neuroscience and the clinical rationale for attention-based pain interventions.
The Two Layers of Pain: Sensation and Suffering
Nociceptive input (the neural signal generated by tissue events) and the subjective experience of pain (the signal plus evaluation, resistance, and emotional response) are neurologically distinct processes. The former is processed in the somatosensory cortex; the latter involves the insular cortex, anterior cingulate cortex, and amygdala. Separating these two layers — attending to the sensation while observing the response to it — is the mechanism through which mindfulness-based pain interventions operate. Kabat-Zinn’s MBSR research with chronic pain patients demonstrated the clinical effects of this separation.
Epictetus and the Distinction Between Event and Judgment
The Stoic philosopher Epictetus wrote in the Enchiridion that some things are within our power and some are not — and that the suffering produced by not distinguishing between these two is the source of most human difficulty. The pain signal from the leg is not within our power. The evaluation of it, and the response to it, are. What Epictetus described as a philosophical distinction two thousand years ago, gate control theory describes as a neurological fact, and this practice makes available as direct experience. The language differs across these three framings. The territory is the same.
Nociception and Pain Experience: The Non-Correspondence
Nociceptive input and subjective pain experience do not correspond in a fixed ratio. The soldier who doesn’t notice a wound; pain that intensifies under anxiety and diminishes under distraction; placebo analgesia — these are expressions of the gate mechanism and central sensitization. Observing pain during meditation is an opportunity to encounter this non-correspondence directly: the signal is present, and its translation into suffering is a variable process that can be observed rather than simply undergone.
Defusion
When this is unbearable or I have to move right now arrives as a verdict during sitting, recognizing it as a thought rather than an accurate assessment of the sensation — and returning attention to the specific, observable characteristics of what is actually being felt — is defusion applied to the evaluative response that physical discomfort reliably generates.