Introduction: Why the Fear of Something Inevitable Weighs So Much

The moment of noticing the grey hair or the new lines in the mirror. The morning when the tiredness takes longer to lift. The low unease while waiting for test results. Aging and illness are changes no one escapes. But the weight of the fear they produce is not entirely explained by the changes themselves.
Much of the fear of aging does not come from the body changing. It comes from the evaluations that arrived from outside and took up residence inside.
Session 1: Why Aging Looks Like Failure

The fear of aging is not a pure response to physical decline. It emerges from the state in which the value of the self has become fused with the condition of the body — specifically, with a body that meets certain standards of youth, vitality, and productivity.
Where does this evaluation come from? In a culture that treats youth as virtue and positions productivity and physical capability as the primary markers of worth, aging registers as deviation from the standard. Grey hair, declining stamina, and changing appearance are read not as natural processes but as evidence of insufficient management or inadequate effort. The anti-aging industry doesn’t only sell products. It continuously reinstalls the premise that aging is something to be prevented, delayed, or corrected — a premise that enters daily life through advertising, wellness culture, and the visual language of what is considered desirable.
The deeper problem is that this evaluation becomes internal. It stops being something delivered by others and becomes something the person delivers to themselves. When looking in the mirror becomes an act of self-assessment, aging stops being a biological process and becomes a recurring audit. The fear of aging is not the fear of the body changing. It is the fear of what a changed body will mean about the person who inhabits it.
Session 2: Practice — Moving From Audit to Companionship
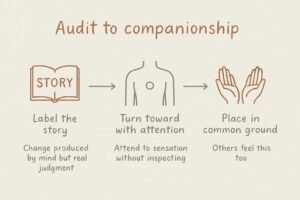
This practice is not aimed at eliminating the fear of aging. It is about gradually shifting the relationship with the body — from the ongoing audit of whether it meets an external standard toward something closer to coexistence with a body that is always in the process of changing.
STEP 1: Label the Story
When the thought arrives — more grey, less stamina, not what it used to be — pause before being pulled into its content.
My mind is running the decline narrative right now.
The change is real. The interpretation — this change is a failure — is a story, not a fact. Observing the story as a generated pattern rather than a verdict creates the first gap in the automatic audit. The body is changing. The judgment about what that change means is something the mind is producing, not something the body is reporting.
STEP 2: Turn Toward One Part of the Body With Attention Rather Than Inspection
Direct attention toward a part of the body that has been producing discomfort or self-criticism — not to evaluate it, but to observe it.
There is a sensation here. This part has been working for a long time.
Without judgment, simply confirm what is present. Allow a moment to register what this part of the body has done across the years it has been functioning. This is not a gratitude exercise in the performance sense. It is a small reorientation of attention — from the critic’s gaze to the observer’s — which changes the quality of the relationship slightly each time it is practiced.
STEP 3: Place the Experience in Common Ground
When the fear of aging or dissatisfaction with the body intensifies, bring it briefly into a wider frame.
What I’m feeling right now, someone else is feeling too — in this city, in many cities, at this same moment.
This is not consolation. It is the recognition that the experience of aging, and the fear and self-criticism it can produce, is not a personal deficiency. It is part of what it means to have a body and to live in a culture with particular standards about what bodies should be. That recognition — however briefly held — is the beginning of self-compassion, which is not self-indulgence but the simple refusal to treat one’s own difficulty as uniquely deserved.
Session 3: The Fear Arrived From Outside
The Stereotype That Got Inside
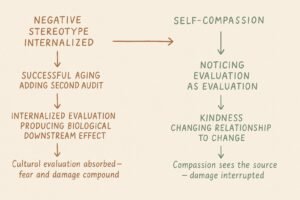
Psychologist Becca Levy’s research on aging demonstrates that the internalization of negative age-related stereotypes produces measurable effects on the biological process of aging itself. People who hold more positive self-perceptions of aging show slower rates of memory decline, lower cardiovascular risk, and longer average lifespans — differences that persist after controlling for initial health status, socioeconomic position, and other confounding variables. The implication is significant: the fear and disgust that can accompany noticing one’s own aging are not neutral emotional reactions. They are the internalization of a cultural evaluation — old bodies are lesser bodies — and that internalization has downstream effects on the very processes it is responding to. The anxiety felt when looking in the mirror is not evidence of weakness or excessive sensitivity. It is evidence of living inside a culture that has systematically associated aging with diminishment, and having absorbed that association before it could be examined.
The New Standard Added to the Old Fear
The structure of aging-related pressure has become more complex in recent decades. The older cultural message was straightforward: aging is decline, and decline is to be feared and concealed. The contemporary cultural message has added a second layer. The framework of successful aging — the ideal of remaining active, productive, socially engaged, and cognitively sharp across the lifespan — repositions aging as a manageable project with its own performance criteria. The framework appears progressive on its surface. But it generates a second audit. In addition to the fear of aging itself, there is now the fear of aging inadequately — of failing to meet the standard of the successfully aging person. This is the aging-specific version of the wellness trap: a system in which there is always a correct way to be doing what the body is already doing involuntarily, and always the possibility of doing it wrong. The person inside the body becomes responsible for its outcomes.
What Kindness Did That Criticism Couldn’t
Psychologist Kristin Neff’s research on self-compassion — defined as comprising three components: self-kindness, recognition of common humanity, and mindfulness — documents its effects on the relationship between self-criticism and physical and psychological wellbeing. People with higher levels of self-criticism show stronger associations between aging anxiety and body dissatisfaction. Self-compassion operates in the opposite direction: treating one’s own aging not as personal failure but as part of the shared experience of having a human body reduces the intensity of the fear and changes the quality of engagement with physical change. Considered alongside Levy’s findings on internalized ageism, self-compassion is not merely a psychological coping strategy. The internalized evaluation — an aging body is a lesser body — is what Levy showed causes the damage. Self-compassion is the capacity to notice that evaluation as an evaluation rather than a fact, and to respond to the self with something other than the criticism the culture provided. It requires only the willingness to treat one’s own difficulty as something other than evidence of personal failure.
Conclusion: The Standard Was Never Neutral

Levy’s internalized ageism will keep producing its effects tomorrow. The successful aging framework will keep offering a new audit to replace the old one. The structure does not change.
But the question am I auditing my body or simply present with it can be asked in front of any mirror, on any morning when the tiredness takes longer to lift. The moment of labeling the decline narrative — noticing that the judgment is a story the mind is running, not a report the body is filing — creates the first distance between the evaluation that arrived from outside and the body that was always just changing.
Aging was never the failure. The standard that made it one was.
KEY TERMS
Internalized Ageism
Becca Levy’s research finding that the internalization of negative age-related stereotypes produces measurable effects on memory decline, cardiovascular risk, and lifespan — independent of initial health status. The fear and self-criticism accompanying awareness of one’s own aging are not neutral emotional responses but the downstream effects of having absorbed a cultural equation between aging and diminishment. The fear of aging reframed as the consequence of an external evaluation that took up residence inside.
Successful Aging
The contemporary framework that repositions aging as a manageable project with performance criteria — active, productive, cognitively preserved, socially engaged — generating a second normative pressure alongside the older fear of decline itself. The aging-specific version of the wellness trap: a system in which there is always a correct way to be doing what the body is already doing involuntarily, and always the possibility of doing it inadequately. Dual normative pressure as the characteristic structure of contemporary aging experience.
Self-Compassion
Kristin Neff’s framework comprising self-kindness, recognition of common humanity, and mindfulness — documented to reduce the association between aging anxiety and body dissatisfaction in ways that self-criticism cannot. Not self-indulgence but the capacity to treat one’s own difficulty as part of shared human experience rather than personal deficiency. In the context of internalized ageism, self-compassion functions as the ability to notice the cultural evaluation as an evaluation — and to respond with something other than the judgment the culture supplied.
Dual Normative Pressure
The condition produced when the older cultural message — aging is decline to be feared — is joined by the newer framework of successful aging, creating a structure in which there is no neutral position. Failing to age is the old fear; failing to age correctly is the new one. The body becomes a project subject to audit from both directions simultaneously, with no configuration that escapes evaluation.
Defusion
The capacity to notice that the decline narrative — this change is evidence of failure — has fused with the experience of observing the aging body, and to receive it as a story the mind is generating rather than a fact the body is reporting. Labeling the narrative creates the first distance between the external evaluation and the present physical reality, making a different quality of attention available.